
The sound of a birth complication lingering in silence is a limp, motionless arm: the stillness of damaged nerves. In Nigeria, neonatal brachial plexus injury (BPI) is no longer just an unpredictable delivery room accident—it is a full-blown public health crisis that is systematically robbing thousands of newborns of their future physical independence while healthcare systems look the other way.
"When my son was born, I noticed his right arm just hung by his side, completely still. The traditional birth attendant told us it was a spiritual attack and that we should rub herbal oils. Months passed, and nothing changed. It wasn’t until we visited a specialist in Ibadan that we learned his nerves were torn during a difficult delivery. With early physical therapy and a custom resting splint, he is finally starting to lift his hand. He is not fully cured, but his future is no longer trapped. — Amina, Oyo"
While medical centers default to passive observation and families resort to ineffective traditional rubs, a simple, highly effective intervention remains virtually invisible in Nigerian postnatal clinical pathways: early neonatal physical therapy and specialized orthotic splinting. Brachial plexus injuries affect a significant percentage of newborns delivered during prolonged, obstructed labors—frequently driven by macrosomia (large birth weight), inadequate pelvic measurements, and limited access to timely cesarean deliveries. Yet, the typical patient trajectory moves directly from missed early detection to permanent, lifelong nerve contractures and physical immobility. We are ignoring a neurological solution to a mechanical birth injury. Early structural mobilization and splinting work by physically preventing joint contractures and protecting the denervated muscles, providing immediate structural preservation that passive waiting can never replicate.
The Three Structural Barriers: Why Nigerian Infants Continue to Suffer
To understand why thousands of Nigerian children remain burdened by a treatable nerve injury, we must look at the three system failures that keep specialized rehabilitative solutions out of reach. These are the discrete truths that dictate the daily struggle of the affected family.
| The Barrier | The Impact on the Patient | The OrthoNarra Mandate |
|---|---|---|
| The Passive Observational Bias | Infants miss the critical first three months of neuroplastic recovery due to "wait and see" advice. | Retraining midwives and pediatricians to mandate immediate referral to pediatric therapy units. |
| The Cost of Specialized Care | Custom neonatal splints and continuous private physical therapy sessions are priced far beyond minimum wage families. | Establishing subsidized, regional pediatric orthotic programs using local lightweight moldable plastics. |
| The Spiritualized Resignation | Families misinterpret nerve damage as a spiritual curse, delaying medical diagnosis until muscles permanently atrophy. | Community advocacy demonstrating that early anatomical alignment and physical engineering restore limbs. |
"Early orthotic splinting and physical therapy do mechanically what neural regeneration requires structurally: they preserve the path for the nerve to reconnect. In Nigeria, waiting for advanced nerve grafting surgery is a luxury for the 1%; immediate conservative physical management is the common-sense solution for the 99%."
The Mechanics of Relief: How Early Intervention Changes the Equation
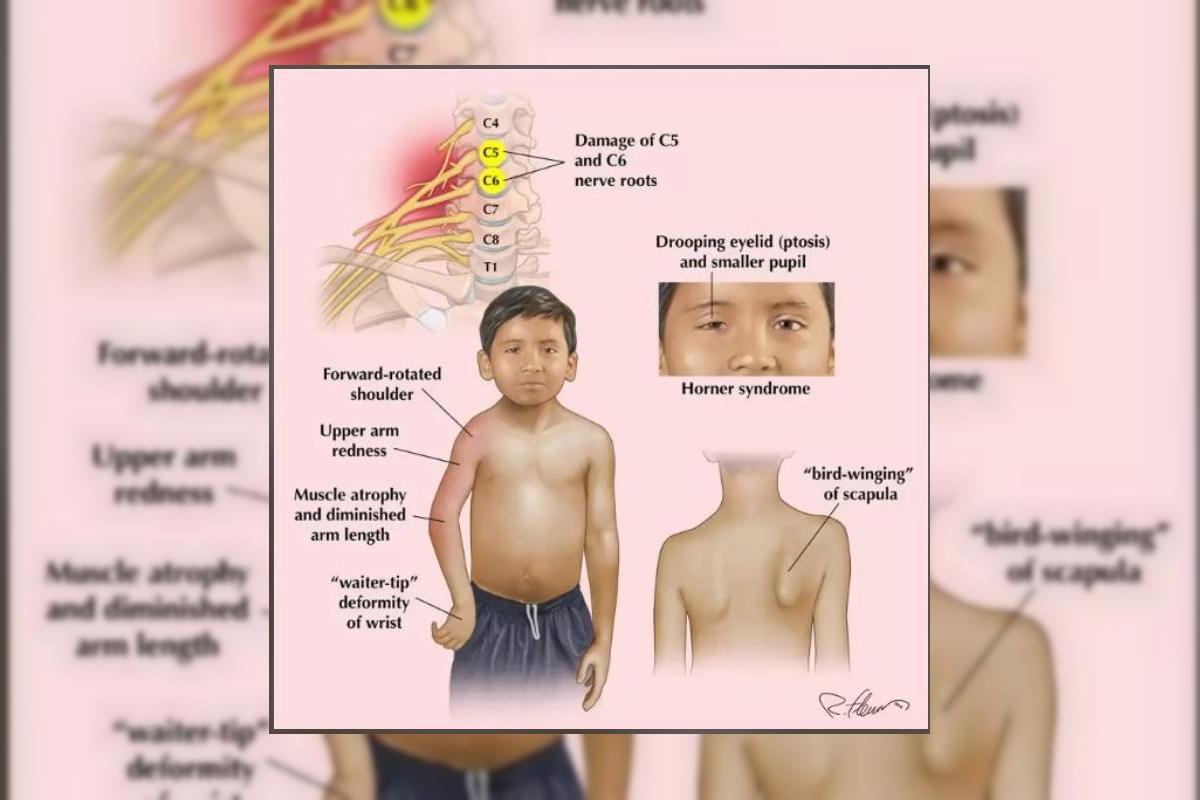
Most brachial plexus injuries in Nigerian newborns present as Erb’s Palsy, affecting the upper nerve roots (C5 and C6) of the network that controls the shoulder, arm, and hand. This causes the classic "waiter's tip" deformity, where the arm hangs limp, rotated inward, with the wrist flexed backward. As the damaged nerves struggle to send signals, the healthy opposing muscles pull tightly, freezing the joint. This is where an **early orthotic splint** and structured movement change everything. By maintaining the arm in a neutral, functional position and applying gentle passive stretching, the intervention acts as a protective shield against joint contractures. The results are foundational: muscle length is maintained, joint subluxation is prevented, and the internal healing environment is stabilized. It is not magic; it is basic neuro-anatomy applied directly to infant development.
The Five Concrete Benefits of Early Neuro-Orthotic Intervention
When an orthotic and therapeutic protocol is introduced during the first weeks of life, it yields five undeniable clinical and socio-economic outcomes:
1 Prevention of Fixed Contractures
By positioning the limb correctly, customized resting splints prevent muscles and tendons from permanently shortening, keeping the joints flexible for future nerve recovery.
2 Protection Against Secondary Dislocation
Muscle imbalance frequently pulls the infant's fragile shoulder joint backward out of its socket. Early stabilizing exercises preserve shoulder structural integrity.
3 Optimization of Brain Neuroplasticity
An infant's brain adapts rapidly. Early tactile and moving stimulation to the affected arm prevents the brain from "forgetting" the limb, preserving sensory-motor pathways.
4 Bypassing Complex Micro-Surgeries
For many infants with moderate nerve stretch injuries, strict conservative management allows the nerves to recover naturally, eliminating the need for expensive, unavailable neuro-grafting.
5 Lifting the Generational Caregiver Burden
A child who recovers full bilateral hand function is a child who grows up to attend school independently, participate in the workforce, and live without requiring lifelong dependent support from aging parents.
The Medical Blindspot: Passive Waiting vs. Mechanical Alignment
The deep forest green and terracotta palette of this series reflects our return to functional, grounded solutions. We must transition away from the institutional reliance on passive observation toward proactive, mechanical support that respects the body’s natural architecture.
| The Observational Loop (The Present) | The Orthotic Pathway (The Future) |
|---|---|
| Telling anxious parents to "wait and see if it heals." | Prescribing a protective resting splint in the first week of life. |
| Passive muscle wasting and permanent joint freezing. | Active joint mobilization and preservation of range of motion. |
| Delayed, desperate seeking of unverified traditional alternative cures. | Continued clinical physical therapy, protecting neuromuscular pathways. |
| Exorbitant lifetime economic costs on long-term disability support. | A minor early investment in durable pediatric orthotic management. |
The current clinical status quo in Nigeria is unacceptable. We cannot allow thousands of our children to grow up with paralyzed limbs, confined by a lack of early care, simply because our medical system views neonatal therapy as a secondary afterthought rather than a primary medical emergency. Brachial plexus injury is an anatomical failure, and anatomical failures require engineering solutions. It is time to reform our delivery room protocols, train our midwives in neonatal upper-limb screening, and make early pediatric splinting as routine as newborn vaccinations.
A Call to Action
To the parents: A limp arm after birth is not an unfixable spiritual affliction; demand to see a pediatric physiotherapist and orthotic specialist before the first month slips away. To the clinicians: Look beyond basic survival; evaluate the spontaneous movement of every newborn's arm before discharging them from the maternity ward. To the policymakers: Subsidizing early intervention neonatal therapy equipment across local government clinics will save families from catastrophic long-term dependency. The terracotta in our palette is the dust of our land, but it is also the foundation we walk upon. OrthoNarra will keep pushing the boundaries of medical education until every affected Nigerian child has the chance to stand firm and use both hands with dignity. Mobility is the bedrock of our independence.



Comments (0)
No comments yet. Be the first!
Please login to leave a comment
Login to Comment