
The destruction begins in absolute silence. In Nigeria, where diabetes is quietly sweeping through families unnoticed, a catastrophic complication is flattening the arches of thousands of feet—not with a sudden impact, but with the terrifying absence of pain.
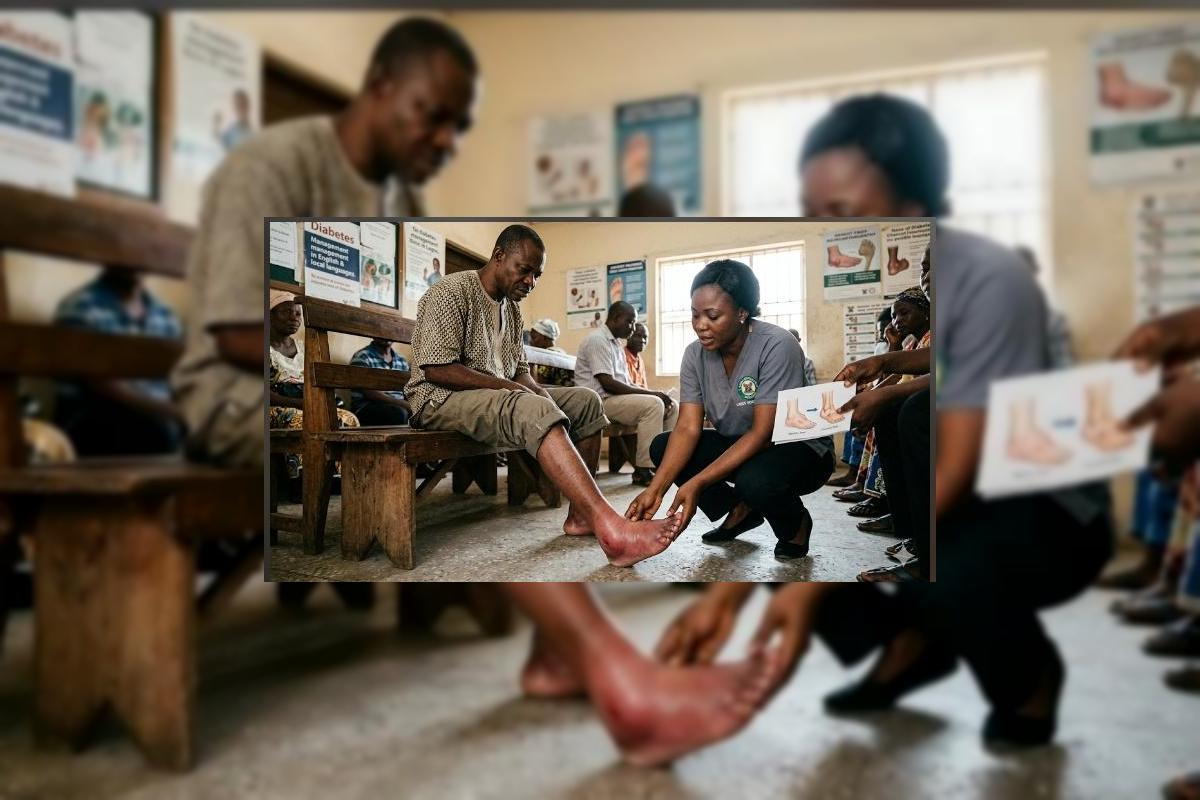
"My left foot became red and swollen like a sponge. I went to the chemist, and he gave me antibiotics, thinking it was an infection. I kept walking on it because it didn’t hurt. Six months later, the bottom of my foot looked like a rocking chair. The bones had completely collapsed. If someone had just told me that a hot, swollen foot without pain is an emergency, I would still be walking normally today. — Ibrahim, Kaduna"
In the landscape of diabetic care across Nigeria, we are facing an information vacuum that costs patients their limbs. While clinics routinely warn diabetics about open sores and ulcers, almost no one is explaining Charcot neuroarthropathy—commonly known as Charcot Foot. This condition is a progressive, destructive disease of the joints and bones, triggered by diabetic nerve damage (neuropathy). Because the nerve fibers no longer transmit pain signals, micro-fractures in the foot go completely unnoticed. The patient continues to walk, crushing their own skeletal structure with every step. We are treating Charcot foot as an infection or a spiritual attack, when it is actually an acute mechanical collapse that requires immediate immobilization.
The Three Fatal Misunderstandings: Why Nigerian Diabetics Lose Their Feet
To stop the preventable epidemic of amputations caused by Charcot Foot, we must dismantle the three fatal misunderstandings that dominate Nigerian communities and primary healthcare centers.
| The Misunderstanding | The Reality of the Disease | The OrthoNarra Mandate |
|---|---|---|
| "If it doesn't hurt, it isn't serious." | The lack of pain is the exact trap; neuropathy masks severe bone fracturing. | Teaching patients that redness and heat are active emergencies, even without pain. |
| The Antibiotic Misdiagnosis | Chemists and clinics misdiagnose the redness as cellulitis, wasting critical weeks on drugs. | Mandatory training for peripheral health workers on Charcot presentation. |
| Traditional Massage & Setting | Taking a fragile, fracturing diabetic foot to a traditional bone setter completely pulverizes the bone. | Absolute prohibition of aggressive physical manipulation on diabetic extremities. |
"Walking on an acute Charcot foot is like driving a vehicle on a shattered wheel. In Nigeria, the average time between the onset of Charcot symptoms and a correct diagnosis is twenty-four weeks—by then, the foot is already permanently deformed."
The Anatomy of Collapse: From Heat to "Rocker-Bottom"
Charcot foot advances through distinct phases, and catching it in the first phase is the only way to save the foot's shape. It starts with an uncontrolled inflammatory response: the foot increases in temperature, swells, and looks flushed. Internally, the bones are losing calcium and softening. If the patient is forced into non-weight-bearing status immediately, the bones can heal cleanly. But when a Nigerian patient walks through the market on a softening foot, the tarsal and metatarsal bones snap and shift. The arch collapses entirely, creating a protrusion under the sole known as a "rocker-bottom" deformity. This protrusion creates localized pressure points that inevitably break open into deep, bone-deep ulcers that frequently lead to transtibial amputation.
The Five Pillars of Charcot Management in Nigeria
Saving a diabetic foot from Charcot destruction does not require experimental medical procedures; it requires structural discipline and the correct application of orthotic engineering:
1 Total Contact Casting (TCC)
The gold standard for acute Charcot is a specialized, molded cast that redistributes weight away from the foot entirely, forcing the patient to remain off the fragile bone while it solidifies.
2 CROW Walkers (Charcot Restraint Orthotic Walker)
Once the acute swelling goes down, patients must be transitioned into a custom-fabricated, rigid boot that fully locks the ankle and midfoot joints, preventing any bone movement during daily activities.
3 The Daily Skin Temperature Audit
Diabetic patients must be taught to use their hands (or an infrared thermometer) to compare the heat of both feet daily. A temperature difference of more than 2°C is an indicator of early Charcot flare-ups.
4 Custom Accommodative Insoles
For feet that have already developed structural changes, specialized orthotic insoles must be carved out to cradle the deformed arch, reducing the pinpoint pressure that causes deadly ulcers.
5 Aggressive Patient Literacy
Every diabetic clinic across our nation must change its posters. We need clear, visual warnings that show Charcot feet alongside ulcerations, translated into Yoruba, Hausa, Igbo, and Pidgin.
The Shift in Strategy: Prevention vs. Post-Deformity Crisis
The deep forest green and terracotta palette of this tenth series anchors our stance on proactive, structural preservation. We are moving our focus from the cold, high-tech amputation theaters to the earthy reality of early clinical screening and protective orthotic shielding.
| The Current Crisis Path | The OrthoNarra Prevention Path |
|---|---|
| Misdiagnosing Charcot as a soft tissue infection. | Immediate immobilization based on swelling and heat alone. |
| Allowing continued walking, pulverizing structural bones. | Applying Total Contact Casting within 48 hours of detection. |
| Traditional bone pulling, worsening bone displacement. | Custom rigid bracing (CROW boot) to preserve the foot arch. |
| Late-stage ulceration ending in amputation. | A permanent, functional limb and uninterrupted independent walking. |
We must end the silence on Charcot Foot in Nigeria. It is an indictment on our medical community when patients lose their limbs simply because nobody explained that a painless, hot, swollen foot is a sign of bones breaking apart inside. We have the prosthetic and orthotic talent in this country to cast, brace, and protect these vulnerable limbs. What we lack is the collective urgency to screen before the arch drops. Let us stop treating diabetes purely from a vial of insulin; we must begin protecting the structural foundation of the human body.
A Directive to the Community
To the diabetic patients: Inspect your feet with your eyes and your hands every single night—if one foot feels like a boiling pot compared to the other, sit down and do not stand up until you see an orthotist. To the family doctors and nurses: Stop prescribing antibiotics for every swollen diabetic foot; rule out Charcot neuroarthropathy first. To the healthcare leaders: Include custom orthotic care in our national health insurance coverage for diabetes. The terracotta is our reminder of the clay from which we are built, and it is our responsibility to keep that foundation from shattering. OrthoNarra will keep documenting the truth until every diabetic foot in Nigeria stands protected. Awareness is the first step toward survival.



Comments (0)
No comments yet. Be the first!
Please login to leave a comment
Login to Comment