
Developmental Dysplasia of the Hip (DDH) is a silent thief of mobility. In Nigeria, it is a condition that, if caught in the first few months of life, is easily corrected with a simple harness. But if left undetected, it evolves into a permanent, painful disability. We are operating against a biological clock that waits for no one.
"We noticed our baby’s legs didn't spread easily when we changed her diapers, but we thought it was just her personality. We waited. By the time we took her to the orthopaedic center at ten months, the doctors told us the hip socket was already malformed and she would need major surgery. If we had known that the 'Pavlik Harness' could have fixed this in a few weeks when she was a newborn, we would have started that day. — Father of Zara, Abuja"
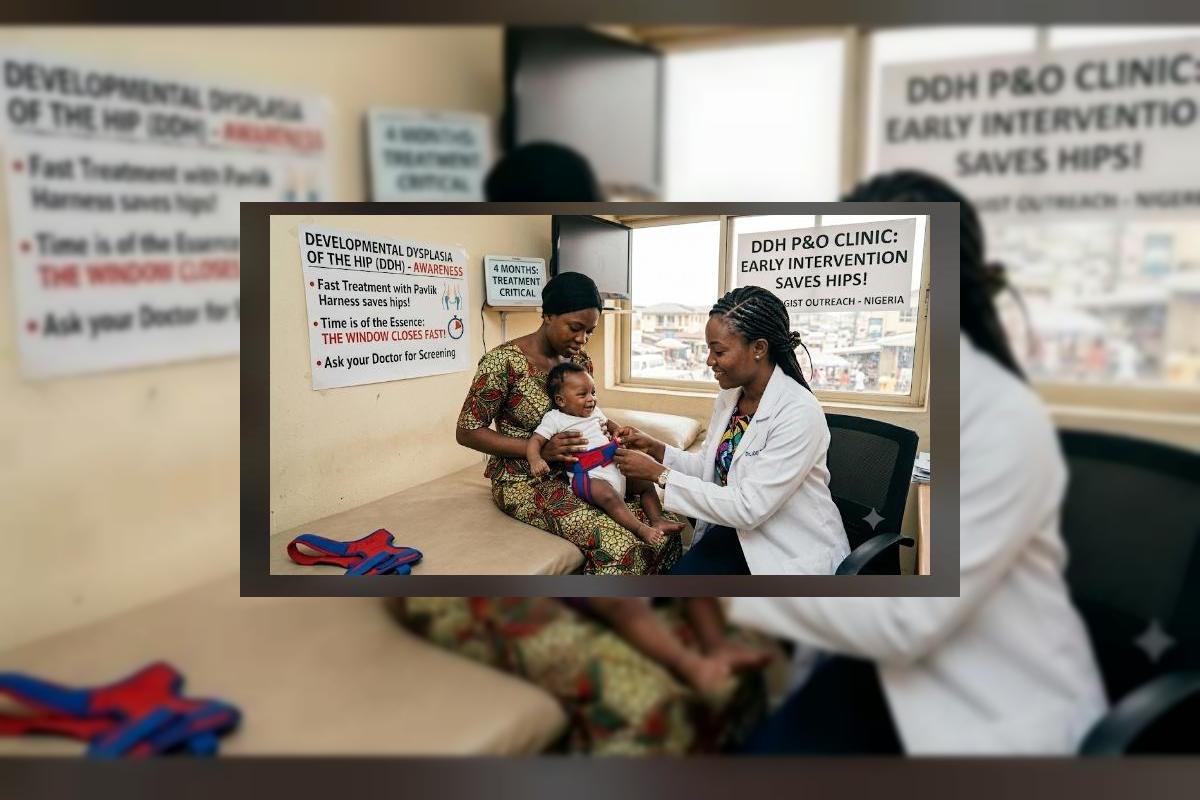
In the landscape of paediatric orthopaedics, DDH is a condition where the hip joint does not form correctly, causing the ball of the thigh bone to sit loosely in the socket. The Pavlik Harness is the gold standard for treatment—a gentle, dynamic bracing system that holds the infant's hips in a flexed, abducted position to encourage the socket to develop normally. The tragedy in the Nigerian context is that DDH is frequently missed during routine postnatal checks, and the "window of opportunity" for non-surgical correction—typically before the age of six months—closes while families are caught in the confusion of seeking traditional, non-medical advice.
The Three Screening Barriers: Why DDH Goes Unseen
To prevent the lifelong consequences of DDH, we must dismantle the barriers that keep this condition hidden in plain sight.
| The Barrier | The Impact on the Child | The OrthoNarra Mandate |
|---|---|---|
| Missed Newborn Checks | Hip instability goes undetected in the critical first weeks. | Mandating Ortolani/Barlow physical tests at every immunization visit. |
| Delayed Parental Concern | Parents wait until the child begins to walk to notice a limp or asymmetrical gait. | Educating parents on "thigh crease asymmetry" and limited hip abduction. |
| Reliance on Traditional 'Setting' | Aggressive manipulation by non-medical bone setters destroys developing cartilage. | Connecting families to trained orthopaedic P&O specialists immediately. |
"The Pavlik Harness works because an infant's bones are like soft wax. By age one, that wax has hardened. In Nigeria, the 'wait-and-see' approach is not cautious—it is a choice to allow a reversible condition to become a lifetime of struggle."
The Mechanics of the Pavlik Harness
The Pavlik Harness is an elegant, non-invasive solution. It consists of a series of straps that gently position the baby’s legs. Unlike a heavy, rigid cast, the harness allows for controlled movement, which is essential for healthy joint development. The goal is to keep the hip socket deep enough to hold the thigh bone in place while the baby grows. When worn consistently as directed by a paediatric orthotist, the success rate for normalizing the hip joint is remarkably high. It is a bridge between a future of potential surgical intervention and a future of natural, normal walking.
The Five Pillars of Early Detection and Treatment
We must normalize the screening process to ensure that no Nigerian child misses the Pavlik window:
1 Neonatal Hip Screening
All newborns should undergo a physical assessment of hip stability by trained medical personnel within the first 72 hours of life.
2 Education on "At-Risk" Signs
Families should be empowered to look for limited hip movement or skin folds that do not match on both legs during dressing and bathing.
3 Accessibility of Ultrasound Diagnostics
In cases of clinical suspicion, an early hip ultrasound is the gold standard for confirmation, providing immediate clarity without radiation.
4 Consistent Harness Protocol
The Pavlik Harness must be fitted by a qualified professional, and parents must be educated on hygiene and monitoring to ensure it stays effective at home.
5 Multidisciplinary Referral
Clear pathways must connect primary health workers to specialized paediatric P&O clinics, ensuring the diagnosis leads to treatment within days, not months.
The Biological Reality: Why Time is the Primary Variable
The shift to forest green and terracotta in this series represents our desire to ground our care in nature and reality. DDH is a developmental process; it is not static. If we do not intervene during the period of rapid growth, the anatomy of the hip changes, and the opportunity for a simple harness treatment vanishes.
| The Late-Diagnosis Path | The Early-Detection Path |
|---|---|
| Missed screening at birth. | Routine hip stability checks at every checkup. |
| Permanent socket deformity. | Normal development via Pavlik Harness. |
| Invasive, expensive surgery. | Non-invasive, low-cost bracing. |
| Early-onset hip arthritis. | Healthy, lifelong joint function. |
The silence around DDH is a tragedy we can fix. By integrating simple hip stability checks into our national postnatal culture, we can virtually eliminate the need for corrective surgeries for this condition. We have the knowledge and the devices to protect the foundation of our children’s mobility. We simply need to make sure the screening happens before the window closes.
A Call for Early Screening
To the parents: Observe your baby's movement—if their legs feel tight or asymmetrical, speak to a doctor immediately; it is better to be safe than sorry. To the healthcare workers: Make hip stability checks a non-negotiable part of your infant physical exams. To the policymakers: Expand access to ultrasound and paediatric orthotic services as a national priority for infant health. The terracotta is the earth our children will walk on—let’s ensure they can walk on it comfortably for the rest of their lives. OrthoNarra will keep the conversation open until early screening is standard across the nation. Mobility is a gift we must protect from the very beginning.



Comments (0)
No comments yet. Be the first!
Please login to leave a comment
Login to Comment