
For Nigerians navigating the loss of a limb or a structural deformity, the road to rehabilitation is split into two distinct paths: the public sector and the private clinic. Choosing between them is often a choice between budget and time, but the hidden cost of this divide is the fragmentation of care itself. Understanding the structural differences is the first step toward getting the help you actually need.
"I went to the teaching hospital first because I thought it was cheaper. The care was good, but the queue was endless—I waited six months just to be measured for a prosthesis. When I finally switched to a private clinic, I paid more, but I had my device in two weeks. I realized then that in our system, you either pay with your money or you pay with your time. — Ibrahim, Kano"
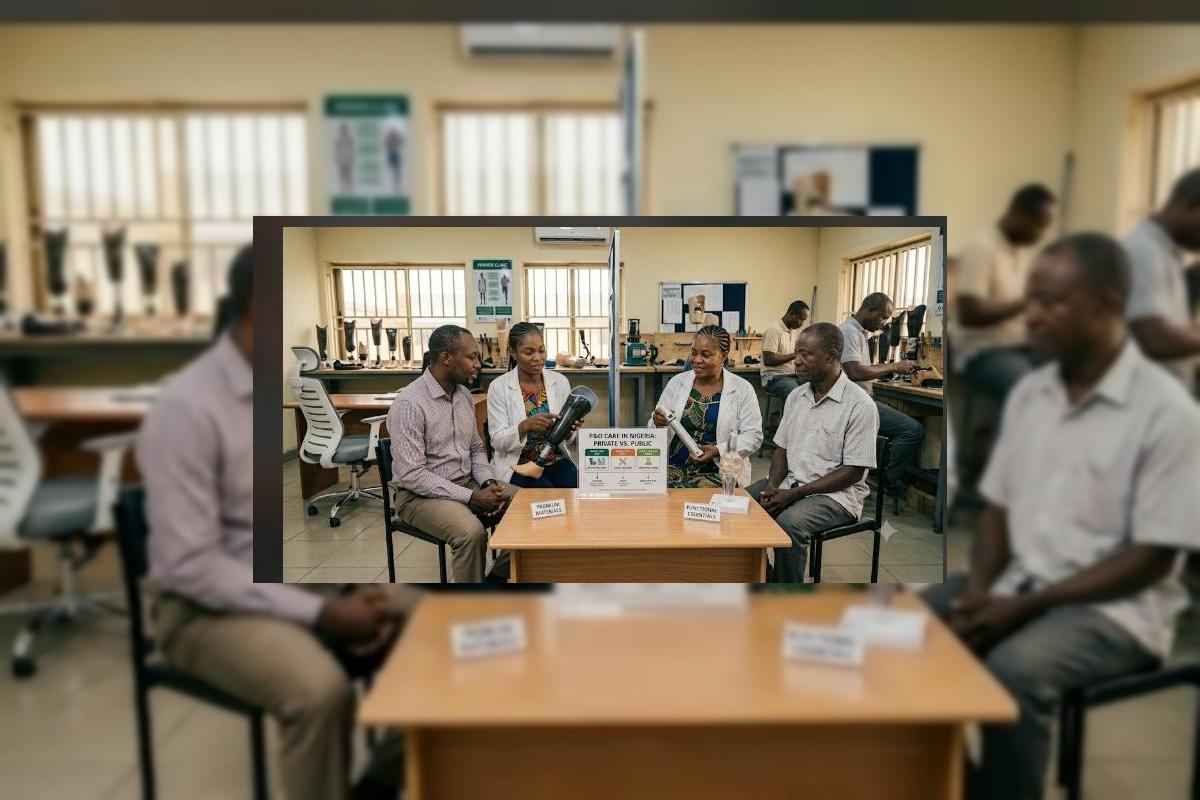
In the Nigerian P&O landscape, the public sector—comprising teaching hospitals and federal medical centers—often serves as the backbone of clinical training and high-volume trauma care. However, they frequently struggle with bureaucratic delays, limited material supply chains, and overwhelming patient-to-clinician ratios. Private practice, on the other hand, offers agility and personalized attention, but the costs can be prohibitive for the average Nigerian family. The gap between these two systems means that many patients either settle for delayed, sub-optimal care or deplete their life savings for expedited services. Bridging this gap is not just about choosing a clinic; it’s about demanding a standard of care that exists in both sectors.
The Three Operational Realities: Comparing Public and Private P&O
Patients need to understand that the "gap" between sectors is defined by three fundamental differences in how clinics operate.
| Operational Factor | Public Sector Reality | Private Sector Reality |
|---|---|---|
| Waiting Time | Extended due to high patient volume and supply delays. | Rapid scheduling for consultations and fittings. |
| Cost Structure | Subsidized, often lower out-of-pocket costs. | Market-rate fees covering specialized overheads. |
| Supply Chain | Centralized procurement, often prone to stockouts. | Flexible, direct ordering from multiple suppliers. |
"A prosthesis is only effective if it arrives during the patient's critical window of neurological adaptation. A public system that makes a patient wait for months is essentially failing the patient, regardless of how professional the clinicians are."
The Cost of the Gap: Why Fragmentation Hurts Everyone
The most dangerous result of this public-private divide is the "rehab drift." Patients often start in the public sector, get frustrated by the wait, and move to private—losing their clinical history and records in the process. This means the prosthetist in the private clinic has to start from scratch, wasting time and money. Furthermore, because private clinics are not fully integrated into the public social welfare net, the most vulnerable patients are often pushed back into the public system, only to start the waiting cycle all over again. The cost of this fragmentation is measured in lost work days, worsening physical health, and the psychological fatigue of being a "patient" instead of a "person."
The Five Rules for Navigating the System
Regardless of where you go, use these five rules to get the best outcome for your rehabilitation.
1 Demand Your Records
Always ask for copies of your clinical notes, measurements, and casting reports. This allows you to move between public and private systems without losing your history.
2 Verify Accreditation
Whether private or public, ensure the lead practitioner is ISPO-accredited or registered with a recognized professional body. Do not compromise on clinical training.
3 Look for Follow-up Protocols
Ask how they handle adjustments. A device that works today will need changes in six months. Ensure the clinic has a plan for long-term maintenance.
4 Clarify "All-In" Pricing
If you are choosing private, ensure the quote includes the socket, the parts, the labor, and at least three follow-up adjustments. Avoid "hidden" costs.
5 Use the Referral Path
Public hospitals often have lists of private clinicians they trust. Ask for a referral rather than searching blindly; it ensures the public system can monitor your outcome.
The Strategic Shift: From Two Islands to One Ecosystem
The deep forest green and terracotta palette reflects our desire for a unified national strategy. We must stop viewing public and private as competitors and start viewing them as complementary parts of a single, functional P&O network.
| The Divided System (Neglect) | The Integrated System (Future) |
|---|---|
| Patients lost in the transfer between systems. | Unified digital records follow the patient. |
| Public and private clinics acting in silos. | Standardized clinical guidelines across both. |
| Private clinics inaccessible to the poor. | NHIA covers costs in accredited private clinics. |
| Stagnation in public supply chains. | Private-Public Partnerships (PPP) for procurement. |
The choice between public and private P&O care should be about convenience, not about the quality of the life-changing device you receive. We must push for a healthcare policy that guarantees the same clinical standard regardless of the building you walk into. Until then, stay informed, guard your medical data, and remember that you are the most important partner in your own rehabilitation team.
A Call to Unified Care
To the patients: You are the bridge; carry your records and advocate for clear treatment plans. To the practitioners: Collaborate across sectors—your shared expertise is the patient's best hope. To the policymakers: Incentivize public-private partnerships so that public hospitals are not overwhelmed and private clinics can serve the marginalized. The.OrthoNarra will keep pushing until rehabilitation is a seamless, national right, not a choice between two worlds. Mobility belongs to everyone.



Comments (0)
No comments yet. Be the first!
Please login to leave a comment
Login to Comment