
The sound of a life interrupted by a stroke is a heavy, rhythmic drag: the sound of a foot scraping against concrete. In Nigeria, adult lower limb spasticity is no longer just an expected complication of neurological survival—it is a full-blown public health crisis that is systematically locking millions of brain injury and stroke survivors out of their communities while healthcare systems treat their physical immobility as an inevitability.
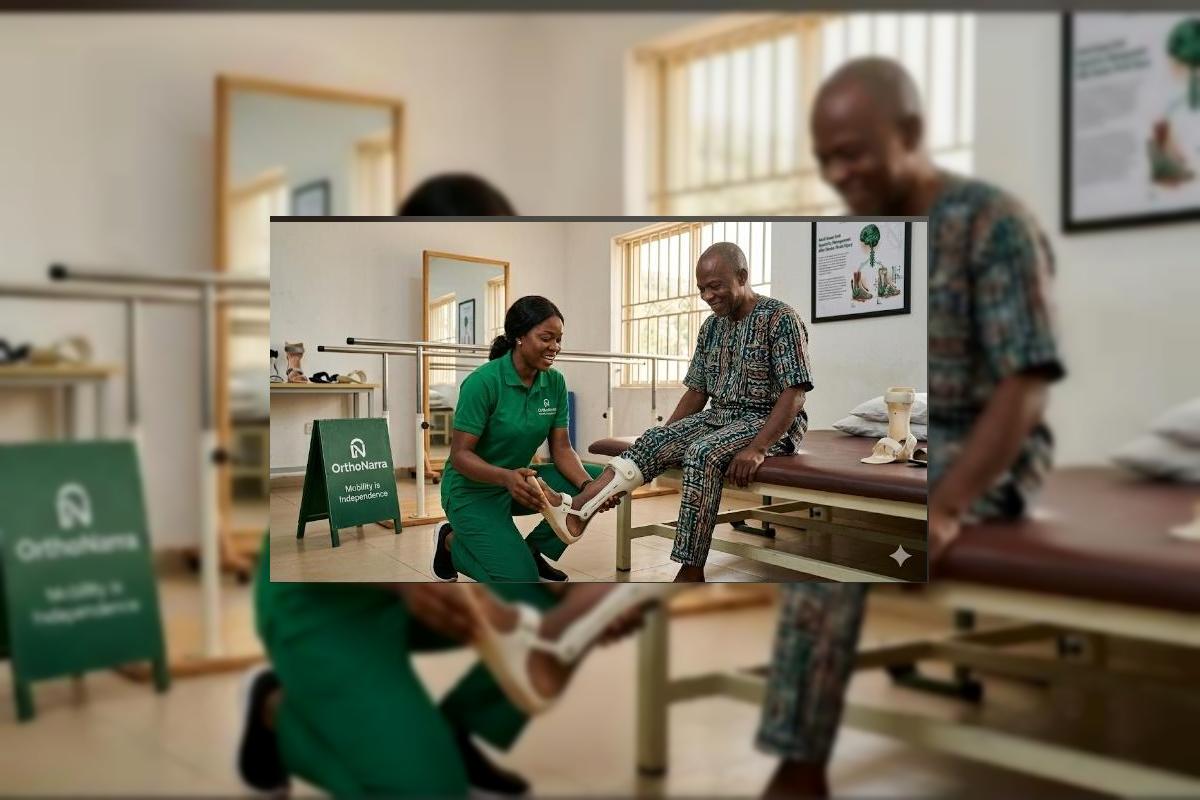
"After my stroke, my high blood pressure was controlled, but my left foot curled inward like a claw. Every step meant dragging my toes on the ground, and the pain in my ankle was blinding. The local clinic told me to keep taking my stroke pills and pray. Then, a specialist fitted me with a rigid 'plastic foot jacket' that fits inside my shoe. The first time I stood up with it, my foot stayed flat. For three years, this brace has kept me walking. I am not completely cured, but I am no longer trapped in a chair. — Baba Olumide, Ibadan"
While medical protocols focus heavily on pharmaceutical management of secondary stroke risks and families drain resources on unverified nerve massages, a fundamental, highly effective intervention remains virtually invisible in Nigerian neurological rehabilitation: the Ankle-Foot Orthosis (AFO). Spastic equinovarus (the spastic foot turning down and inward) affects a massive percentage of Nigerian stroke and traumatic brain injury survivors, driven by a high regional burden of unmanaged hypertension, road traffic accidents, and a lack of early rehabilitation access. Yet, the typical patient trajectory moves directly from the neurology ward to permanent, painful joint contractures and total physical dependence. We are ignoring a mechanical solution to a neurological-mechanical problem. An ankle-foot orthosis works by providing a structural baseline that physically counteracts the hyper-tonic muscle pulling, providing immediate ankle alignment and clearance that no chemical pill can replicate.
The Three Structural Barriers: Why Neuro-Survivors Continue to Drag Their Feet
To understand why millions of Nigerian stroke and brain injury survivors remain homebound by a manageable walking deficit, we must look at the three system failures that keep orthotic solutions out of reach. These are the discrete truths that dictate the daily struggle of the neurological patient.
| The Barrier | The Impact on the Patient | The OrthoNarra Mandate |
|---|---|---|
| The Pharmacological Monopoly | Patients are kept on systemically draining muscle relaxants that cause severe drowsiness without physically correcting their walking mechanics. | Educating neuro-rehabilitation teams to prescribe structural bracing simultaneously with medical spasticity management. |
| The Centralization of Orthotic Labs | Custom, lightweight polypropylene AFOs are only fabricated in a few distant tertiary teaching hospitals, leaving rural patients stranded. | Establishing localized clinical hubs equipped with modular, heat-moldable orthotic components for rapid, affordable fitting. |
| The "Stroke Destined" Resignation | Communities accept a dragging foot and permanent bedrest as the natural, unalterable fate of surviving a brain injury. | Launching public awareness campaigns demonstrating that post-stroke mobility can be mechanically preserved and re-engineered. |
"An ankle-foot orthosis does mechanically what damaged brain signals fail to do: it holds the foot flat against gravity to allow a safe step. In Nigeria, waiting for high-end botulinum toxin injections or orthopedic tendon transfers is a luxury for the 1%; distributing functional AFOs is the common-sense solution for the 99%."
The Mechanics of Relief: How the Orthosis Changes the Equation
When a stroke or brain injury damages the central nervous system, the brain loses its ability to control muscle tone. In the lower limb, the calf muscles over-activate, pulling the heel upward while the tibialis posterior muscle forces the sole of the foot to turn inward (spastic equinovarus). When the patient tries to walk, their toes point downward, catching on the ground and creating a severe tripping hazard. This is where the ankle-foot orthosis (AFO) changes everything. By wrapping around the calf and extending under the sole, the brace acts as a rigid or semi-rigid structural lever that locks the ankle at a safe 90-degree angle. The results are immediate: toe-drag is eliminated, the foot is held flat during weight-bearing, and the patient's walking pattern stabilizes. It is not magic; it is basic physics applied directly to neuro-anatomy.
The Five Concrete Benefits of Early Orthotic Intervention
When an orthotic protocol is introduced during the early sub-acute stages of neurological recovery, it yields five undeniable clinical and socio-economic outcomes:
1 Immediate Prevention of Falls
By clearing the toes from catching on the ground during the swing phase of walking, the brace significantly reduces catastrophic fall risks and subsequent bone fractures in fragile stroke survivors.
2 Halting Fixed Joint Contractures
Continuous spasticity causes muscles and tendons to permanently shorten into hard, unyielding deformities. An AFO provides a constant, gentle stretch that keeps tissues elongated and joints pliable.
3 Reduction of Compensatory Pain
To avoid tripping on a dragging foot, patients are forced to hike their hips upward or swing their leg outward (circumduction). A brace normalizes the gait, protecting the lower back and hips from severe structural wear.
4 Accelerating Brain Re-education
Walking with a flat, stable foot sends clear sensory feedback up into the brain. This consistent neural messaging is vital for neuroplasticity, helping the brain rebuild damaged walking pathways far more effectively.
5 Restoration of Social and Economic Autonomy
A stroke survivor who can walk safely is an individual who can return to their place of worship, look after their household, and access their workplace without requiring a constant, full-time family caregiver.
The Medical Blindspot: Passive Medication vs. Mechanical Alignment
The deep forest green and terracotta palette of this series reflects our return to functional, grounded solutions. We must transition away from the institutional reliance on lifelong sedentary medication toward structural, mechanical support that respects the body’s natural architecture.
| The Passive Medical Loop (The Present) | The Orthotic Pathway (The Future) |
|---|---|
| Prescribing heavy sedating pills that ignore the physical foot drop. | Fitting a rigid or dynamic AFO alongside early neuro-physiotherapy. |
| Allowing the ankle tendon to shorten permanently into a fixed claw-foot. | Continuous structural alignment to preserve ankle flexibility and calf length. |
| Severe exhaustion and body tilt caused by hip-hiking and leg swinging. | Energy-efficient walking with proper heel strike and toe clearance. |
| Exorbitant lifetime expenditure on continuous care and dependency resources. | A definitive investment in a structural device that restores walking independence. |
The current clinical status quo in Nigeria is unacceptable. We cannot allow millions of our resilient neuro-survivors to be confined to beds and backrooms, watching their mobility waste away, simply because our medical system treats orthoses as secondary rehabilitation accessories rather than essential medical interventions. Lower limb spasticity is a structural control failure, and structural control failures require engineering solutions. It is time to reform our post-stroke clinical pathways, train our community doctors in orthotic screening, and make ankle-foot orthoses as basic and accessible as walking sticks.
A Call to Action
To the survivors and families: A turning, dragging foot after a stroke is not a life sentence to a chair; demand to see a prosthetic and orthotic specialist before the joint freezes permanently. To the physicians: Look past the prescription pad; check your patient’s ankle alignment during their standing check-ups and refer them for bracing early. To the policymakers: Integrating orthotic manufacturing and evaluation into primary healthcare programs will save billions in long-term family care costs and socio-economic dependency. The terracotta in our palette is the dust of our land, but it is also the foundation we walk upon. OrthoNarra will keep pushing the boundaries of medical education until every limping neuro-survivor in Nigeria has the chance to stand firm, lift their foot, and walk with dignity. Mobility is the bedrock of our independence.



Comments (0)
No comments yet. Be the first!
Please login to leave a comment
Login to Comment