
Foot drop is one of the most common and most disabling complications of stroke in Nigeria. A simple ankle-foot orthosis can restore safe walking within weeks. Most survivors never hear about it.
"My husband survived the stroke. He can think clearly, he can speak, he remembers us. But he shuffles when he walks and his foot catches the ground and we are terrified every day that he will fall. Three hospitals. Not one person mentioned a brace.Wife of a stroke survivor, 61 years old · Asaba, Delta State"
Nigeria loses approximately 200,000 people to stroke every year. Many more survive and among those survivors, a significant proportion are left with a problem that is immediately visible, daily disabling, and almost entirely correctable: they cannot lift the front of their foot when they walk. Every step becomes a hazard. Every staircase becomes a threat. The medical term is foot drop. The orthotic solution is ankle foot orthosis. The gap between these two facts in Nigerian hospitals, in Nigerian homes is enormous.
What Foot Drop Actually Is
Stroke damages the brain pathways that control voluntary movement. When the area governing dorsiflexion the upward lifting of the foot is affected, the muscles responsible for that movement become weak or paralysed. The foot hangs downward during the swing phase of walking. To clear the ground, the patient must hike their hip unnaturally high, swing the leg wide, or drag the toe. This compensatory gait is exhausting, inefficient, and carries a serious fall risk. In a country where most homes have uneven floors, open compounds, and no assistive infrastructure, that fall risk is not abstract.
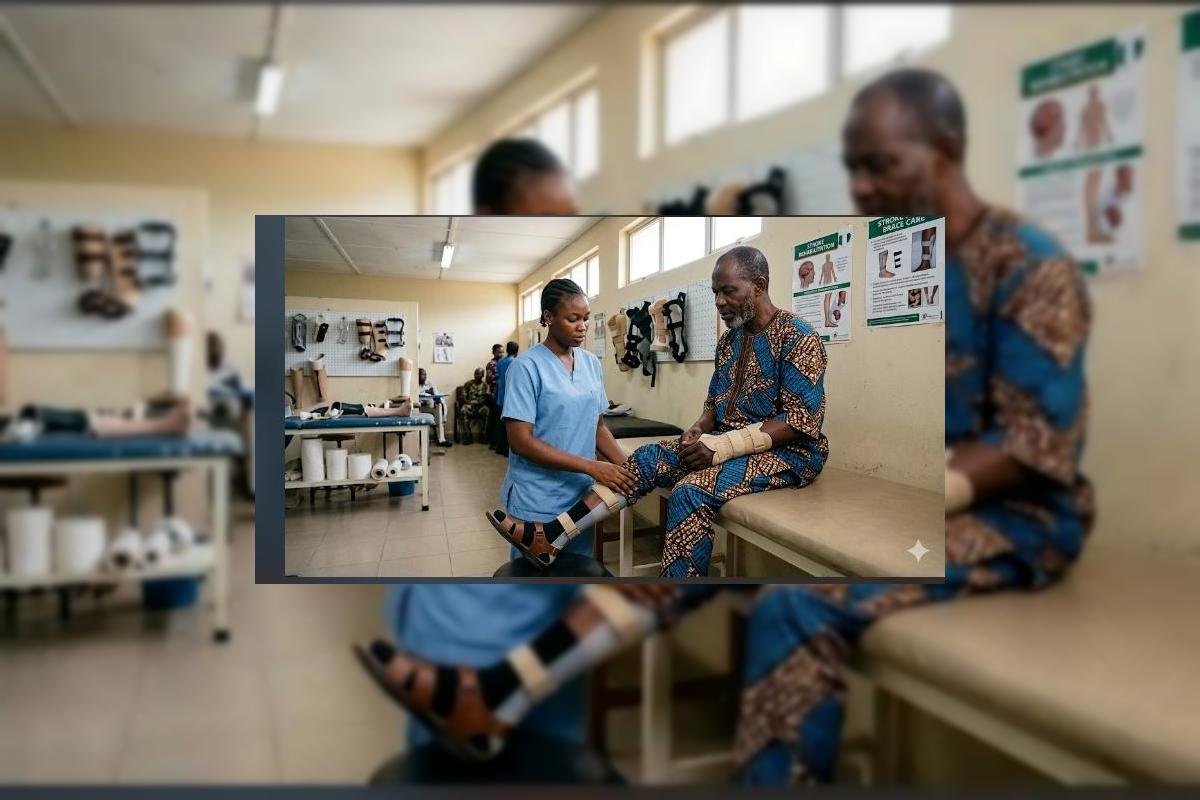
"The foot hangs. The toe drags. Every step is a negotiation between the person and the ground. A correctly fitted AFO eliminates that negotiation in most cases, within the first week of use."
The AFO: Simple, Effective, Overlooked
The ankle foot orthosis (AFO) is a lightweight plastic splint that holds the foot and ankle at a functional angle typically 90 degrees during walking. It fits inside a shoe. It is fabricated from thermoplastic material, custom moulded to the patient's leg. It does not cure the neurological damage from the stroke. What it does is provide the mechanical substitute for what the weakened muscles can no longer do: hold the foot up, clear the ground, and allow a safe, efficient gait pattern.
Without AFO
Toe drag, compensatory hip hike, high fall risk. Abnormal gait stresses hip and knee joints. The patient avoids walking, leading to rapid deconditioning, isolation, and depression.
With Correctly Fitted AFO
Safe, functional walking within days of fitting. Reduced fall risk. Normal shoe wear. Improved confidence, independence, community participation, and long term rehabilitation outcomes.
The evidence for AFO use in post stroke foot drop is among the strongest in all of neurorehabilitation. It is listed as a standard intervention in stroke care guidelines across the UK, USA, Europe, and the WHO rehabilitation framework. In Nigeria, it remains largely unknown to patients and, in many settings, unreferenced by the clinicians treating them.
What Stroke Families Must Do Now
1 Name the problem at the next clinic visit
Tell your doctor or physiotherapist specifically: "His foot drops when he walks." Ask directly whether an ankle-foot orthosis is appropriate. Use those words. Many families describe the symptom vaguely; naming it precisely activates a different clinical response.
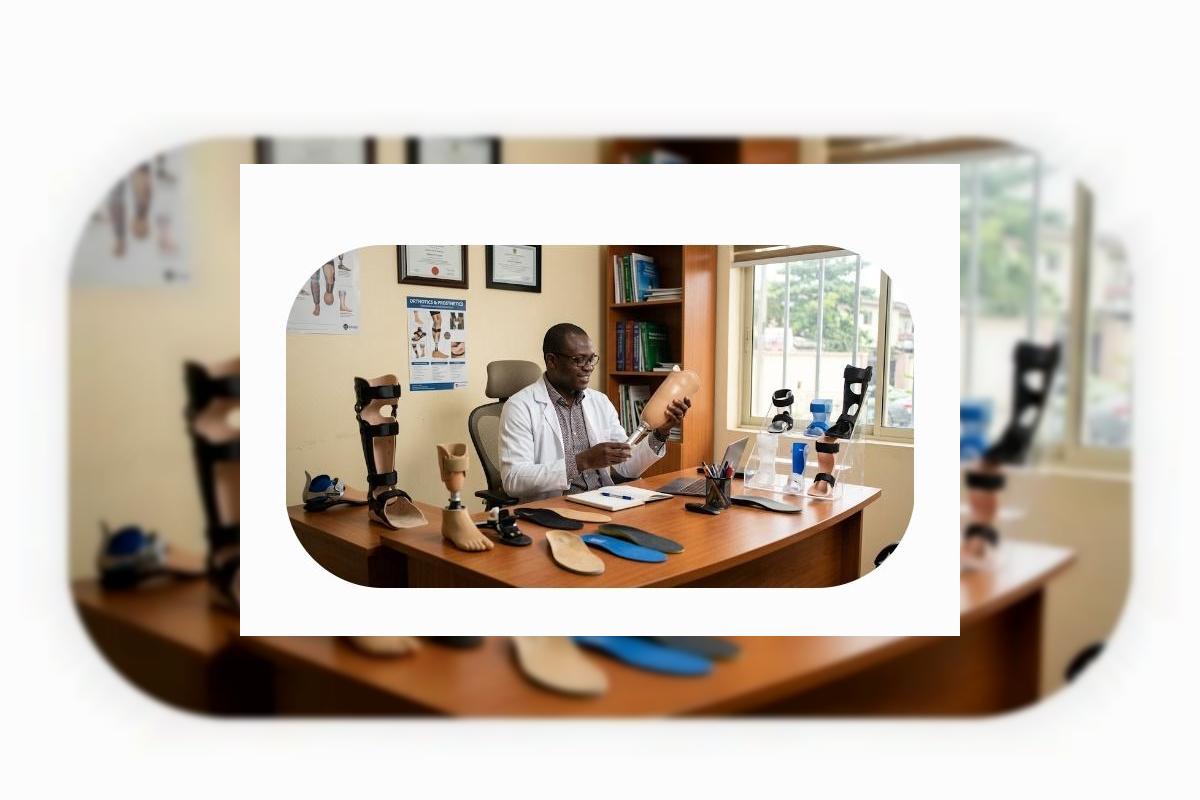
2 Request a P&O referral not just physiotherapy
Physiotherapy addresses muscle strength and movement re-education. A prosthetist or orthotist assesses and fabricates the AFO. Both are needed. Ask for both. In most Nigerian hospitals with a P&O unit, an AFO can be fabricated within days of referral.
3 Do not buy a generic brace from a pharmacy
Off the shelf braces sold in pharmacies and markets are not substitutes for custom-fitted AFOs. A poorly fitted orthosis can cause pressure sores, worsen gait, and reduce compliance. Custom fabrication by a trained orthotist is not a luxury it is the functional standard.
4 Start as early as possible
AFO intervention is most impactful in the first three to six months post-stroke, when neuroplasticity is at its peak and gait patterns are still forming. Early fitting shapes recovery. Delayed fitting manages a pattern that has already set. The difference in outcomes is significant.
Stroke rehabilitation in Nigeria is underfunded, fragmented, and rarely multidisciplinary in any meaningful way. Neurologists manage the acute event. Physiotherapists manage movement. But the prosthetist the professional whose device could give a survivor back their walking is almost never part of the conversation. That must change, hospital by hospital, referral pathway by referral pathway, until the AFO is as automatically discussed after a stroke as the blood pressure medication.
For Stroke Families
If someone in your home is living with a post stroke foot drop and has never been assessed for an AFO, that assessment is overdue. Contact the P&O unit at your nearest teaching hospital or Federal Medical Centre. Ask for an orthotist. Describe the foot drop. Bring the patient. The brace that could restore their walking may be closer, simpler, and more affordable than you have been led to believe because nobody has led you there at all. Ortho Narra is here to change that.



Comments (0)
No comments yet. Be the first!
Please login to leave a comment
Login to Comment