
"They cut off my leg on a Thursday. By Saturday I was discharged. Nobody mentioned a prosthesis. Nobody mentioned physiotherapy. The doctor said come back in six weeks for wound review. That was the last time anyone in that hospital spoke to me about my leg"
Emmanuel's Story
He had known about his diabetes for eleven years. He took his medication when the pharmacy had it, when the cost was manageable, when life permitted. He checked his feet sometimes. He saw his doctor when symptoms demanded it. He was not negligent; he was a fifty eight year old man in Warri managing a chronic condition in a healthcare system that gave him a prescription and sent him home, with no structured diabetic foot screening programme, no specialist nurse, no podiatry service, and no one whose job it was to catch the thing that was quietly coming for him.
The wound on the sole of his right foot started as a blister. He did not feel it from diabetic peripheral neuropathy had stolen most of the sensation from his feet years earlier. By the time his wife noticed it while helping him bathe, it had been there for at least two weeks. By the time they reached the hospital, it was infected. By the time the infection was assessed, bone was involved. The surgeon removed his leg below the knee three days later.
Emmanuel's amputation was not inevitable. It was the end product of a long chain of missed interventions any one of which, caught in time, could have broken that chain. That chain is what this article is about.
Nigeria's Diabetes Amputation Crisis, by the Numbers
The International Diabetes Federation estimated Nigeria's diabetic population at over 11 million people in 2021 a figure that has likely risen since, given population growth and the continued urbanization, dietary shift, and physical inactivity that are driving type 2 diabetes rates across sub-Saharan Africa. Nigeria now carries the largest absolute burden of diabetes on the continent.
11M+Nigerians with diabetes (2021)
60% Undiagnosed or poorly controlled at any time
25% Of surgical beds in major Nigerian hospitals diabetic foot complications
5% Who receive structured prosthetic rehab post amputation.
Diabetic foot disease the collective term for foot ulcers, infections, and neuropathic and vascular complications of the diabetic foot is the leading cause of non-traumatic lower limb amputation in Nigeria. Studies across Nigerian teaching hospitals consistently show diabetic foot complications occupying a disproportionate share of surgical admissions: some reports estimate up to 25% of general surgical ward beds at any given time are occupied by patients with diabetic foot disease. It is one of the most resource consuming conditions in Nigerian surgery and simultaneously one of the most preventable.
"Diabetic foot disease consumes up to 25% of surgical beds in Nigerian teaching hospitals yet structured prevention programmes, foot screening clinics, and prosthetic rehabilitation pathways remain almost entirely absent from the public health system."
The Chain That Breaks Every Single Time
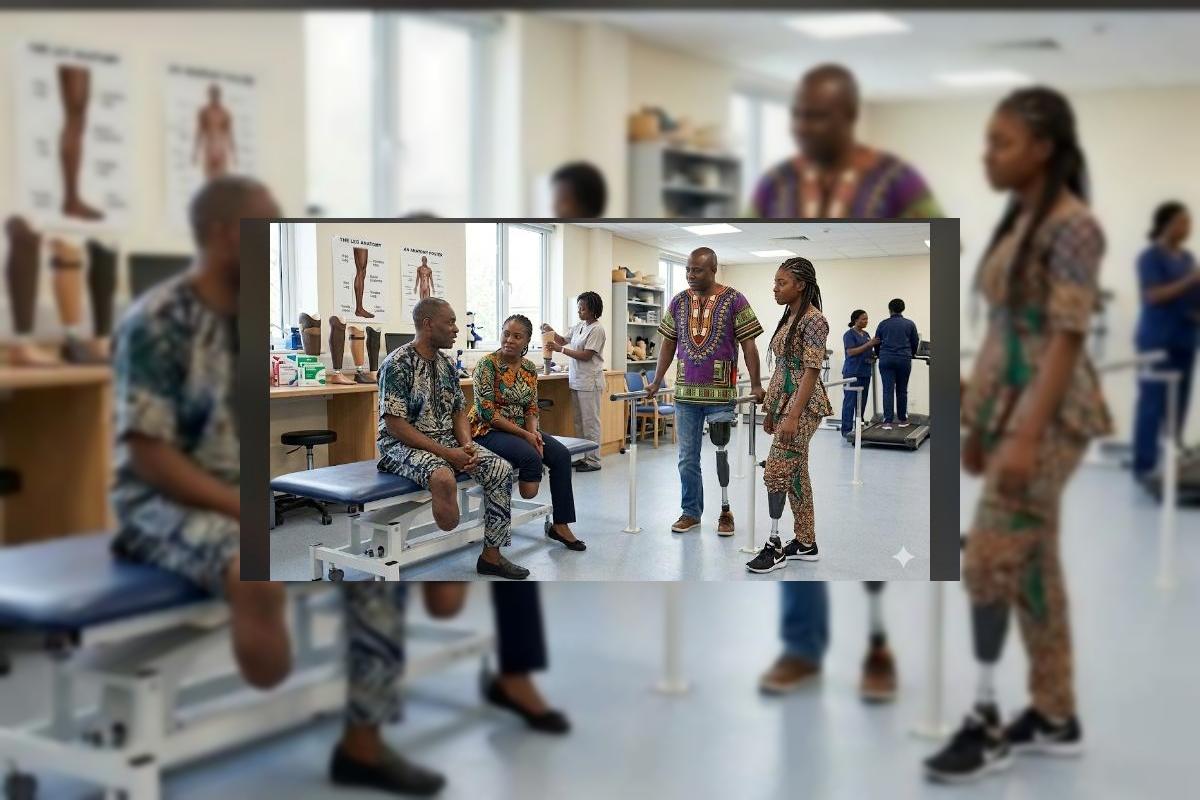
The path from diabetes diagnosis to amputation to rehabilitation passes through multiple clinical contact points each of which represents an opportunity for intervention. In high income countries with structured diabetic care pathways, this chain is managed by multidisciplinary teams: endocrinologists, diabetic nurse educators, vascular surgeons, podiatrists, wound care specialists, prosthetists, and physiotherapists working in coordinated sequence. In Nigeria's public health system, almost none of this coordination exists at scale.
The Diabetic Amputation Pathway Where Nigeria's System Breaks Down
- Diabetes Diagnosis
Often delayed by years. Many patients present at diagnosis with already established complications. No structured follow up protocol in most facilities.
- Foot Screening Gap
Regular diabetic foot screening examining for neuropathy, vascular insufficiency, pressure points is standard of care globally. In Nigeria it is almost entirely absent outside private specialist clinics.
- Ulceration Develops
Neuropathic wounds develop silently. Patients present late often after days or weeks of unnoticed ulceration. Cultural and financial barriers further delay presentation.
- Wound Care Gap
Specialist wound care, offloading devices, and vascular assessment are inconsistently available. Surgical amputation is reached earlier than necessary due to inadequate conservative management.
- Amputation Performed
Surgery is competent in most facilities. The stump is closed. The patient is stabilised. Medical care at this stage is adequate but it is also the last structured care most patients receive.
- Rehabilitation Void
No P&O referral. No physiotherapy pathway. No prosthetic assessment. Patients are discharged with wound care instructions and a follow-up date. The rest rebuilding a life is left entirely to them.
Why Diabetic Patients Lose Limbs; The Six Factors
Diabetic amputation is rarely a single event with a single cause. It is the convergence of multiple, interacting pathological processes each of which is manageable if caught early, and catastrophic if missed until late. Practitioners and patients alike need to understand what drives this cascade
- Peripheral Neuropathy
- Peripheral Arterial Disease
- Foot Deformity & Pressure
- Poor Glycaemic Control
- Footwear & Walking Surface
- Delayed Presentation
- A ten minute examination monofilament testing for neuropathy, ankle-brachial index for vascular assessment, foot inspection for deformity and pressure points identifies at risk patients before wounds develop. This is the single highest yield intervention in diabetic foot prevention and it requires no specialised equipment beyond a monofilament and a trained examiner.
- Custom or prefabricated diabetic footwear wider toe boxes, cushioned insoles, no internal seams dramatically reduces ulcer recurrence in high-risk patients. In Nigeria, diabetic footwear prescription remains almost entirely in the private sector. It should be a standard P&O service in every hospital with a diabetic clinic.
- Patients need to know: inspect your feet daily, report any break in skin immediately, never walk barefoot, keep nails trimmed straight, dry between toes. This knowledge is elementary but in studies across Nigerian teaching hospitals, majority of diabetic patients had received no structured foot care education at any point in their management.
- Every patient discharged following lower limb amputation should have a documented referral to a prosthetics and orthotics service not as an optional note, but as a required component of the discharge process. This single systemic change, requiring no additional resources beyond a referral letter and a pathway, would transform the post-amputation experience for thousands of patients annually.
- No wound care, no orthotic device, and no surgical skill can compensate for chronically uncontrolled diabetes. Nigeria's public health system must treat diabetes medication supply and monitoring access as an infrastructure issue not as the patient's individual financial problem. A patient who cannot afford their insulin cannot protect their feet.
What Must Change And Who Must Change It
The Rehabilitation Void
Studies from Nigerian teaching hospitals report that fewer than 5% of lower limb amputees receive formal prosthetic rehabilitation. The reasons are consistent: absence of P&O referral at discharge, prohibitive device cost, geographic inaccessibility, and absence of post amputation physiotherapy. For a diabetic patient who has already lost a limb, the failure to provide rehabilitation does not merely delay recovery it significantly increases mortality risk. Bilateral immobility, pressure complications, cardiovascular deconditioning, and psychological collapse following amputation are all substantially reduced by timely, adequate prosthetic rehabilitation.
Current Reality
No structured diabetic foot screening in public primary or secondary care
P&O services absent from most diabetic management teams
No mandated P&O referral pathway at amputation discharge
NHIA does not reliably cover prosthetic devices post-amputation
Diabetic footwear unavailable in public health facilities
No national diabetic foot programme or amputation prevention strategy
What Must Be Built
- Annual foot screening at every diabetic clinic monofilament, ABI, inspection
- Prosthetist and orthotist embedded in every hospital diabetic foot team
- Mandatory P&O referral letter as required discharge document post amputation.
- NHIA benefit schedule updated to explicitly cover post amputation devices.
- Therapeutic diabetic footwear as prescribed P&O service at public hospital.
- National diabetic amputation register to drive evidence and policy.
Emmanuel at Sixty
He found his way to a private P&O clinic fourteen months after his amputation, through a connection his nephew made on his behalf. The prosthetist who assessed him found a well-healed residual limb that had been left entirely without rehabilitation no physiotherapy, no strength work, no pre prosthetic conditioning. His contralateral (remaining) foot showed early signs of the same neuropathic changes that had taken his right leg. Nobody in the hospital that discharged him had examined it.
He was fitted with a transtibial prosthesis. He learned to walk again at sixty years old, with the focused determination of a man who understood exactly what he had nearly lost entirely. He now inspects his remaining foot every morning a habit the prosthetist taught him, that eleven years of diabetic follow up appointments had never thought to establish.
Emmanuel's story does not end in tragedy. But it should never have come as close to one as it did. Nigeria has the clinical knowledge, the patient needs, and the human capital in its P&O and medical workforce to do far better than this. What is missing is the systemic will ; the decision, made at the level of hospital protocols, insurance frameworks, and ministry policy to treat the person who survives an amputation as a patient who still deserves a complete course of care.
The silent epidemic will not stay silent forever. It is accumulating in wards, in homes, in the growing number of Nigerians walking on one leg who should be walking on two. Ortho Narra will keep naming it until someone listens.
If you are a Nigerian living with diabetes: examine your feet daily. Report any wound, blister, or discolouration to your doctor immediately do not wait for your next scheduled appointment. If you have never been screened for diabetic neuropathy or peripheral vascular disease, ask for it at your next visit. If you have experienced a lower limb amputation and have not been referred to a prosthetist, you have the right to request that referral. Your rehabilitation is part of your treatment not an afterthought to it.



Comments (0)
No comments yet. Be the first!
Please login to leave a comment
Login to Comment