
The data is not just a warning; it is an indictment. In Nigeria, the gap between the need for prosthetic and orthotic (P&O) services and the professionals available to provide them is no longer a "shortage"—it is a systemic collapse.
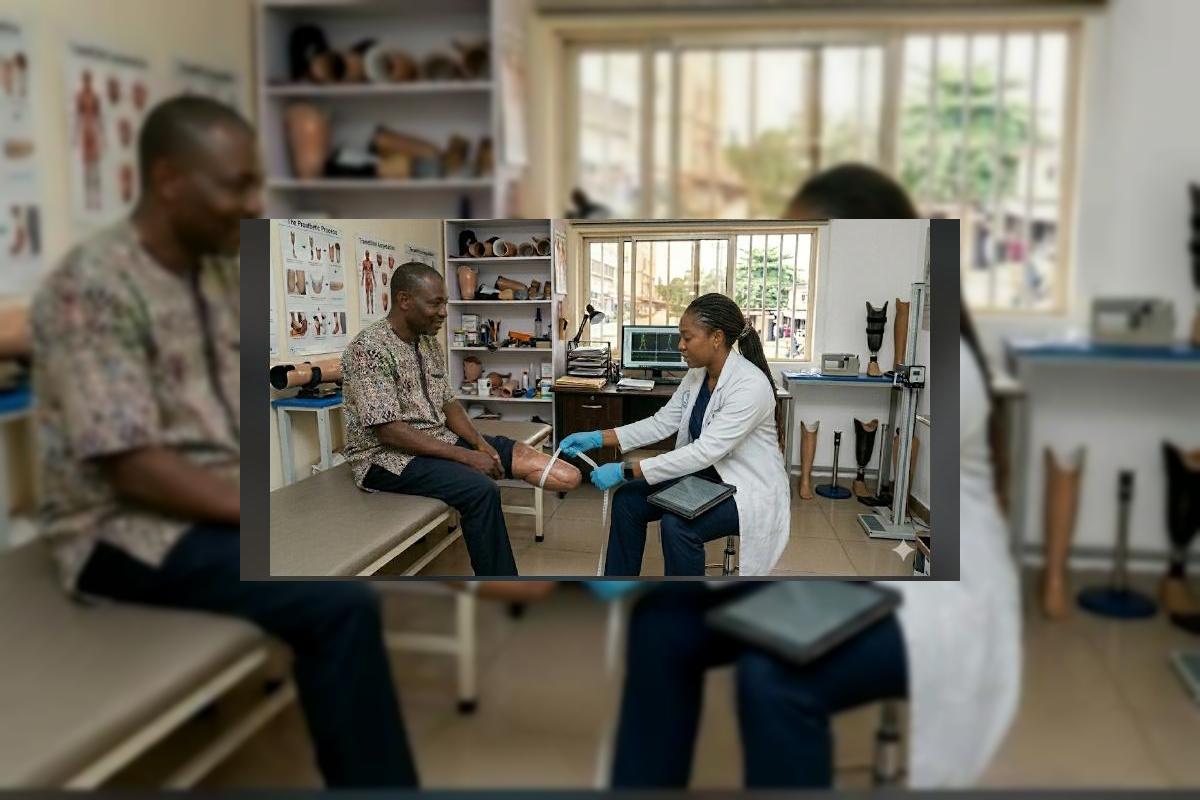
"I graduated in 2022, ready to change lives. But in my clinical placement, I saw 50 patients waiting for two clinicians. We have the passion, but we are being trained in a vacuum. There are no materials, the faculty is stretched thin, and most of my classmates are already looking for visas to practice in the UK or Canada. We are losing the few we actually train. — P&O Graduate, Lagos"
Nigeria currently operates at approximately 2% of the World Health Organization’s recommended minimum for P&O workforce density. While the global standard suggests a ratio closer to 1 practitioner per 5,000 to 10,000 people, Nigeria languishes at a staggering 1:54,000. This is the audit of a crisis. Behind every missing limb and every uncorrected deformity is a missing professional—a vacancy that the current educational and policy framework is failing to fill. We are not just training too few people; we are failing to build the infrastructure required to keep them here. This post is a sharp departure from our previous stories of individual survival. Today, we look at the numbers, and the numbers do not lie.
The Global Comparison: A Continental Audit
When placed side-by-side with our African peers, Nigeria’s investment in workforce development is revealed as dangerously inadequate. While we claim to be the "Giant of Africa," our rehabilitation sector is a shadow of what it should be. The following table illustrates the percentage of the WHO-recommended minimum workforce currently active in each nation. It is a shareable reality check for every healthcare administrator in the country.
| Country | Practitioner to Population Ratio | % of WHO Minimum Floor |
|---|---|---|
| South Africa | 1 : 18,000 | 45% |
| Ghana | 1 : 28,000 | 28% |
| Kenya | 1 : 32,000 | 22% |
| Ethiopia | 1 : 41,000 | 12% |
| Nigeria | 1 : 54,000 | 2% |
"The workforce gap is a silent emergency. Our annual graduate output is a mere 8% of what is required to replace retiring clinicians, let alone expand services to rural populations. The math simply does not add up for a functional future. We are effectively preparing for a future where disability remains permanent because the hands that could fix it have left the country."
The Five Root Causes of the Shortage
To fix the shortage, we must acknowledge the five policy failures that have created it. This is not a lack of interest from students; it is a failure of the system to provide a viable career path. Each of these points represents a discrete lever that policymakers can pull—if they choose to act.
1 Educational Bottlenecks and Accreditation
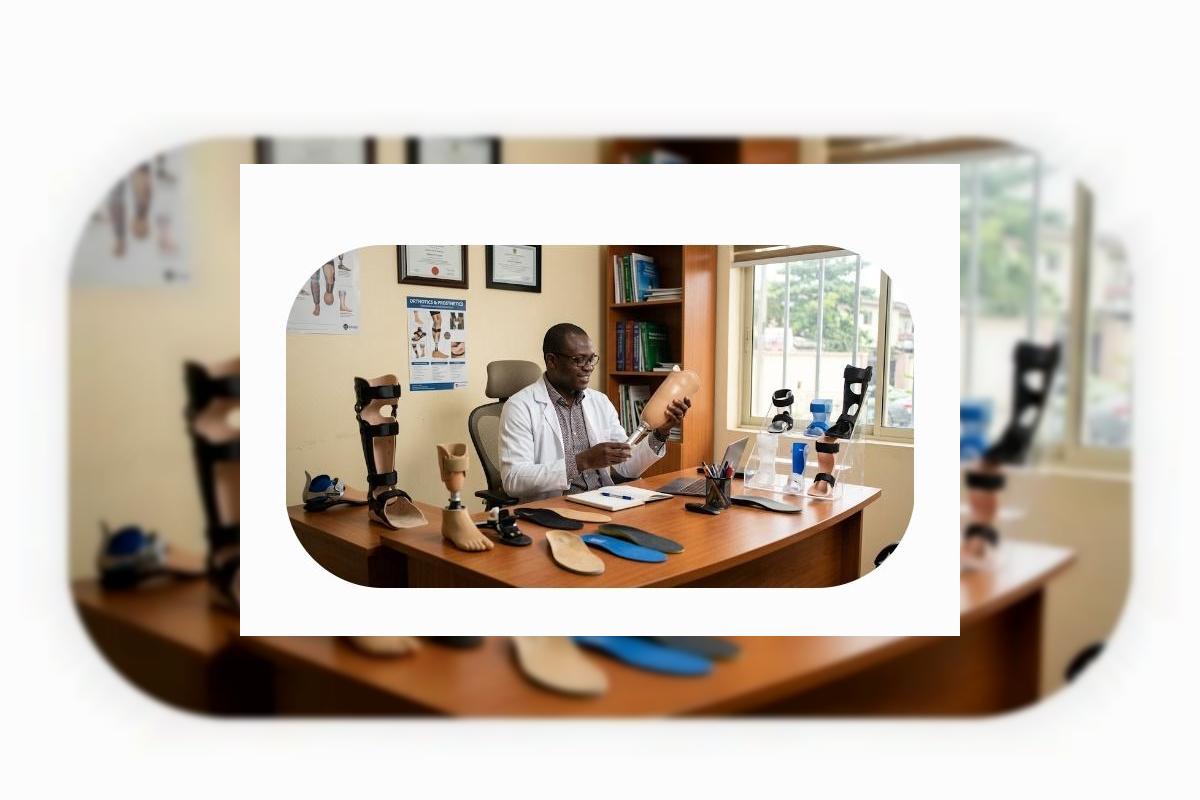
Nigeria has very few accredited institutions capable of training Prosthetists and Orthotists to ISPO (International Society for Prosthetics and Orthotics) standards. Without accreditation, degrees are unrecognized globally, and more importantly, graduates lack the clinical rigor required for complex cases. We need a massive investment in the Federal College of Orthopaedic Technology (FECOT),and similar institutions to double their capacity and modernize their curriculum.
2 The "Brain Drain" of Skilled Technicians
The few high quality graduates we produce are immediately targeted by international recruitment. Without competitive salaries, clear career progression in the civil service, or modern workshops to work in, Nigeria’s best P&O minds are building the workforce of the UK and Middle East instead of their own. We are essentially paying for the education of clinicians who will never treat a single Nigerian patient.
3 Total Absence of Material Subsidies
Training requires consumables- thermoplastics, resins, and carbon fiber. These are almost entirely imported. When the Naira fluctuates, the cost of training a single student doubles. Institutions are forced to teach theory because they cannot afford the "practice." A student who has never laminated a socket or pulled a plastic sheet over a cast is not a clinician; they are a spectator. We need duty-free imports for educational P&O materials.
4 The Policy-Clinical Disconnect
Policymakers often group P&O under general "rehabilitation," failing to realize it is a highly specialized engineering-medical hybrid. Consequently, budget allocations for "equipment" rarely cover the specialized machinery needed to outfit a training lab. The P&O profession needs its own seat at the table in the Ministry of Health, not just a footnote in a physiotherapy budget.
5 Lack of Integrated Referral Pathways
Because there are so few practitioners, many doctors don't know who to refer to. This creates an artificial "low demand" in some regions, which leads to further underfunding. It is a death spiral of visibility. If a surgeon doesn't know a prosthetist exists, they won't refer the patient; if the school doesn't see referrals, they don't see the need to train more students.
Current Reality vs. What Must Be Built
The shift from slate to electric blue in this post's palette is a call to move from the cold reality of today to the high-voltage future we must build. We cannot wait another decade for "gradual improvement."
| Current Reality (The Deficit) | The Mandate (The Future) |
|---|---|
| 1 practitioner per 54,000 citizens. | Scaling to 1:10,000 by 2040. |
| Theory-heavy, material-poor training. | Hands-on, ISPO-accredited clinical residencies. |
| Career stagnation in public hospitals. | Specialist grading for P&O in the civil service. |
| Heavy reliance on imported components. | Local manufacturing of P&O resins and plastics. |
The time for "awareness" has passed. We are now in the era of accountability. Every year we delay the expansion of our P&O schools, thousands of Nigerians—from the stroke survivors on the Lagos-Ibadan expressway to the children with clubfoot in the north—lose their mobility permanently. We are not just missing workers; we are missing the very people who help Nigeria stand on its own two feet. This is a matter of national productivity, human rights, and common sense.
To the Stakeholders
To the students: Stay the course, but demand better facilities. You are the vanguard of a movement. To the practitioners: Your data is your power; document every patient you turn away so the waitlists can no longer be ignored. To the policymakers: The 1:54,000 ratio is a failure you can no longer ignore. If you want a productive, mobile workforce, you must first build the workforce that enables it. The audit is complete. The next step is investment. OrthoNarra will keep the lights on until the dots start turning blue. Mobility is not a luxury—it is the foundation of our nation's progress.



Comments (0)
No comments yet. Be the first!
Please login to leave a comment
Login to Comment